Born in Stuttgart, Germany in 1979, Dr. Dt. Erdem Çetin began his education in Kırşehir and completed his schooling there, from primary school through to high school. He then successfully completed his university education at the Faculty of Dentistry at 19 Mayıs University in Samsun.
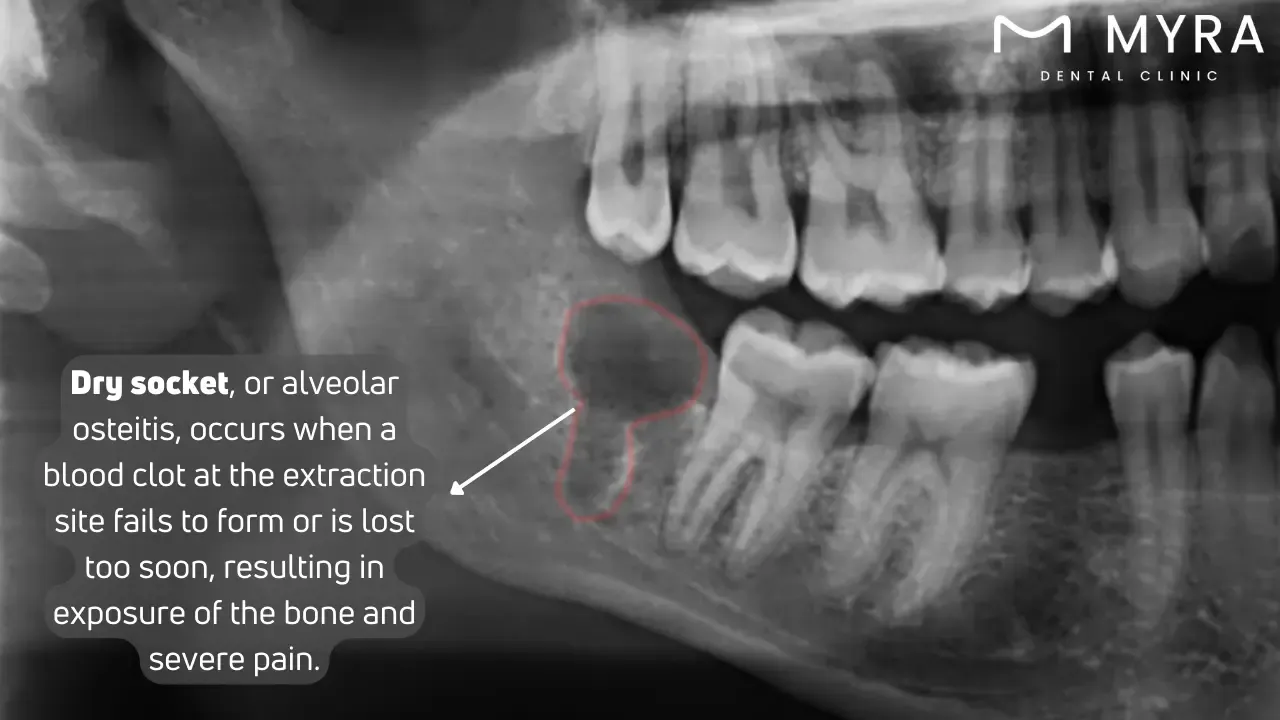
A dry socket, medically termed alveolar osteitis, represents a common yet painful complication following tooth extraction. A blood clot normally forms within the empty socket, the void left in the bone, as the body begins to heal after a tooth is removed. The clot protects the underlying bone and nerves from exposure to air, food particles, and fluids, facilitating proper healing. The protective blood clot does not form adequately or is dislodged too soon, leading to severe pain and complications in dry sockets.
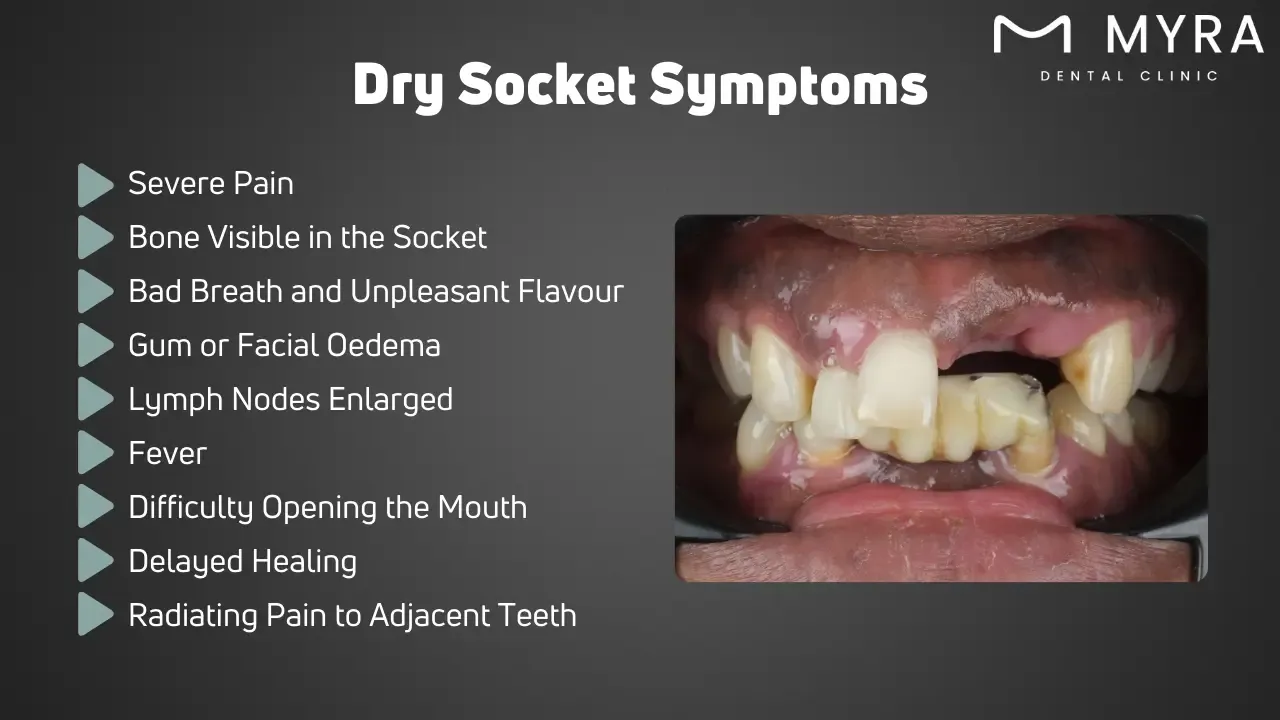
The most prevalent symptom of a dry socket is severe pain that usually starts a few days after extraction and radiates to the ear, eye, or neck on the same side. The extraction site appears empty with visible bone, often whitish in appearance due to exposure. Patients usually experience bad breath and an unpleasant taste in the mouth, resulting from the accumulation of food particles and bacteria in the unprotected socket. Other patients experience swelling of the gums or face and enlarged lymph nodes as the body's inflammatory response to irritation and infection. Patients develop a mild fever, have difficulty opening their mouth (trismus), experience delayed healing, and feel pain radiating to adjacent teeth due to shared nerve pathways.
Effective management of a dry socket requires professional dental intervention. Medicated dressings containing substances like eugenol are applied to the socket to alleviate pain and reduce inflammation. The dentist flushes the socket with a sterile saline solution or antiseptic rinse to remove debris and bacteria. Over-the-counter pain relievers, such as acetaminophen or ibuprofen, help manage severe pain. Antibiotics like amoxicillin or clindamycin treat infections if they are present or likely. Home remedies such as warm saline rinses provide relief but are insufficient for proper treatment.
The dry socket research evaluates various prevention and treatment interventions and understands their causes. The Cochrane Review titled "Local interventions for the management of alveolar osteitis" by Blanaid, et al., found that chlorhexidine mouth rinses and gels significantly reduce the risk of developing dry sockets after tooth extraction. The systematic review "Smoking as a Risk Factor for Dry Socket: A Systematic Review" by Kusnierek, et al. demonstrated that smokers have a more than threefold increased risk of developing dry sockets compared to non-smokers. The review "Management of Dry Socket: New regenerative techniques emerge while old treatment prevails" by Kamal, Omar, and Samsudin identified traditional and regenerative treatment strategies, highlighting the superior efficacy of modern regenerative methods like Platelet-Rich Plasma and laser therapy. The study "Management of dry socket with low-level laser therapy" by Kamal, et al. at the University Dental Hospital Sharjah showed that LLLT significantly lowers pain and accelerates healing in dry socket cases compared to conventional treatments.
What is Dry Socket?
A dry socket, medically termed alveolar osteitis, represents a common yet painful complication following tooth extraction. A blood clot forms within the empty socket, the void left in the bone, as the body begins to heal after a tooth is removed. The blood clot protects the underlying bone and nerves from exposure to air, food particles, and fluids, facilitating proper healing. The clot essentially acts as a biological dressing, promoting tissue regeneration and preventing contaminants from entering the wound site.
The protective blood clot does not form adequately or is dislodged too soon in cases of dry sockets. What does dry socket look like? It appears as an empty-looking socket with exposed bone, with a whitish appearance due to the bone being visible. The premature loss of the clot exposes the bone and nerves, resulting in severe pain that radiates to the ear, eye, or neck on the same face as the extraction.
Early-stage dry socket presents with increasing pain a few days after the extraction rather than subsiding as expected. The exposed bone is empathetic and easily irritates, causing significant discomfort and prolonging healing. Factors contributing to the development of dry sockets include smoking, vigorous rinsing or spitting, trauma at the extraction site, and certain medical conditions or medications that interfere with normal blood clotting. Dry socket is a dental problem which requires professional care and attention.
What are the Types of Dry Socket?
The types of dry sockets are listed below.
Partial Dry Socket: The blood clot that forms in the socket after tooth extraction is partially dislodged or dissolved, common in an early-stage dry socket. A partial dry socket shows some bone exposure, but the clot still covers part of the socket, providing a trim level of protection. Pain and discomfort are present but not as severe as in a full dry socket.
Complete Dry Socket: Complete dry socket occurs when the blood clot is lost from the socket, exposing the bone and nerves fully. A complete dry socket is characterised by intense pain radiating to other parts of the face, head, or neck. The exposed bone is highly susceptible to irritation and infection, causing significant discomfort and delaying healing.
What are Dry Socket Symptoms?
The dry socket symptoms are listed below.
Severe Pain: The most prevalent symptom, severe pain, commences a few days following the extraction or during the early stage dry socket and extends to the neck, eye, or ear. The discomfort results from the heightened sensitivity of the exposed bone and nerves to air, food, and liquids.
Bone Visible in the Socket: The extraction site is described as having a whitish appearance, and the visible bone is vacant. The bone is left unprotected by the absence of a blood clot, which results in increased sensitivity and irritation.
Bad Breath and Unpleasant Flavour: Halitosis (bad breath) and a foul flavour in the mouth are experienced by patients. It results from the accumulation of food particles and microbes in the unprotected socket, which results in infection and odour.
Gum or Facial Oedema: Certain patients experience swelling near the extraction site or in the facial region. The body's inflammatory response to irritation and infection in the exposed socket is the cause of the enlargement.
Lymph Nodes Enlarged: Lymph nodes in the neck or mandible region may experience swelling. The enlargement is a reaction to infection or inflammation, as the body's immune system endeavours to combat microorganisms in the exposed socket.
Fever: Mild fever develops in patients as a systemic response to infection, as the body attempts to combat microorganisms in the open socket.
Difficulty Opening the Mouth (Trismus): Patients experience difficulty completely opening their mouths. The trismus condition is attributed to muscle contractions and inflammation near the extraction site.
Delayed Healing: The healing process is substantially slowed in the presence of a dry socket. New tissue formation is impeded in the absence of the protective blood clot, exacerbating recovery.
Radiating Pain to Adjacent Teeth: The sensation of multiple teeth being affected is exacerbated by the pain that extends to adjacent teeth. The phenomenon results from the shared nerve pathways in the mandible, which results in referred pain from the exposed socket.
What are the Causes Dry Socket?
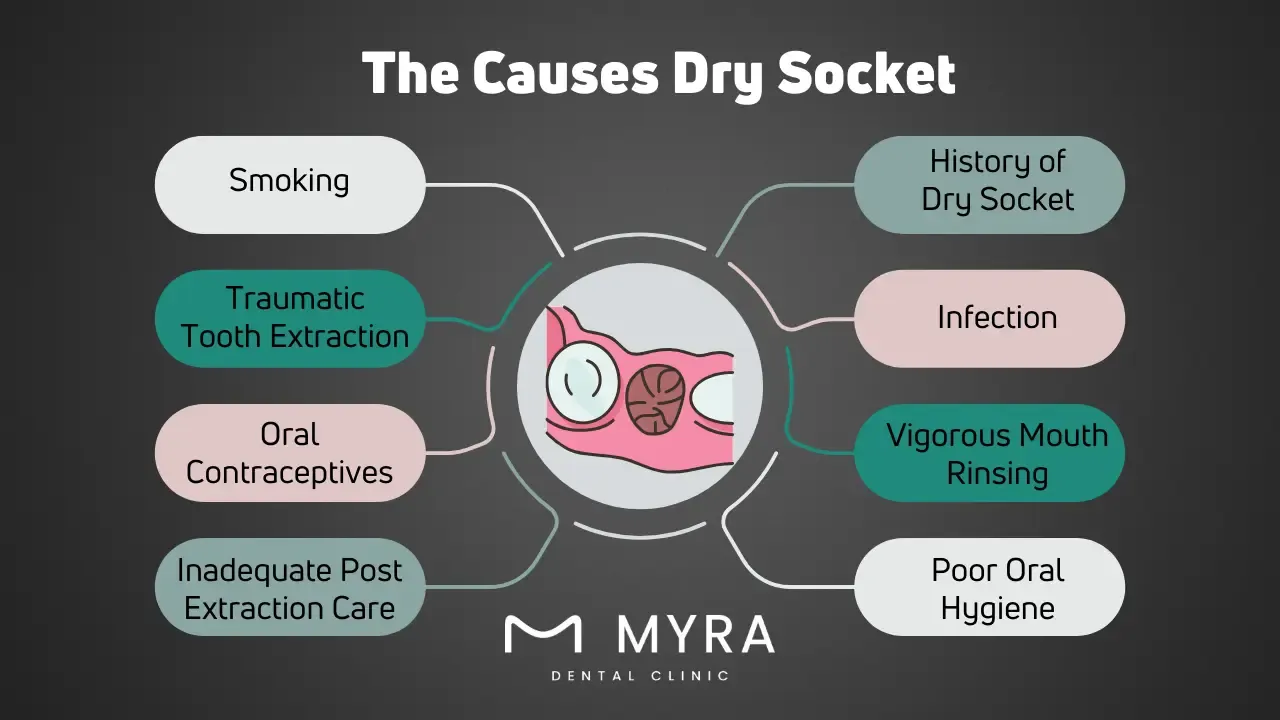
The causes of dry socket are listed below.
Smoking: The risk of dry sockets is substantially elevated by smoking, as it reduces the blood supply to the gums and impedes the formation of clots. The blood clot is prematurely dislodged by the inhaling motion while smoking, which can expose the bone and nerves.
Traumatic Tooth Extraction: A dry socket results from complex or challenging extractions, such as extractions that involve impacted teeth. The proper formation and stability of clots are impeded by excessive manipulation and damage to the adjacent bone and tissue.
Oral Contraceptives: The normal blood coagulation process is disrupted by the high estrogen levels that oral contraceptives produce. The hormonal influence results in unstable or incomplete blood coagulation, which increases the socket's susceptibility to exposure.
Inadequate Post-Extraction Care: A dry socket results from failing to follow aftercare instructions, such as not delicately rinsing the mouth or avoiding specific foods. The socket is exposed if the thrombus is dislodged or dissolved due to inadequate care.
History of Dry Socket: Patients who have previously experienced dry socket are at an increased risk of developing it again. The predisposition is attributed to oral environment factors that impede correct clot formation or differences in healing responses.
Infection: Pre-existing infections near the extraction site impeding a stable blood clot formation. Bacteria cause the clot to decompose or disintegrate, revealing the underlying bone and nerves.
Vigorous Mouth Rinsing or Swallowing: The forming blood clot is dislodged by excessive rinsing or swallowing immediately following an extraction, which is common for early stage dry socket. The mechanical disruption obstructs the clot from stabilising and safeguarding the socket.
Poor Oral Hygiene: Bacteria accumulation in the mouth results from neglecting oral hygiene. The risk of dry sockets is increased by high bacterial levels, which interfere with blood clot formation and increase the likelihood of the clot breaking down.
What are the Treatments of Dry Socket?
The treatments of a dry socket are listed below.
Medicated Dressings: Dentists apply medicated dressings containing eugenol or other analgesic substances directly to the dry socket to alleviate discomfort and reduce inflammation, especially for early stage dry socket. The dressings protect the exposed bone and nerves, fostering a more favourable environment for healing.
Flushing the Socket: The dentist irrigates the socket with a sterile saline solution or an antiseptic rinse to remove debris, food particles, and bacteria on the site of tooth extraction. The purifying process mitigates the risk of infection and alleviates irritation, facilitating the socket's healing process.
Pain Medication: Over-the-counter pain relievers such as acetaminophen or ibuprofen alleviate the severe pain associated with dry sockets. These medications contribute to the patient's comfort during healing by reducing inflammation and providing analgesic effects.
Antibiotics: Antibiotics, including amoxicillin and clindamycin, are prescribed when an infection is present or there is a high risk of developing one. These antibiotics prevent further complications and eliminate bacterial infections, facilitating the healing of the exposed cavity.
Can Dry Socket Be Treated At Home?
No, a dry socket cannot be treated at home. Professional dental intervention is essential for effectively managing and treating dry sockets. A dry socket necessitates the thorough debridement of the socket, the application of medicated dressings, and the potential prescription of analgesics and antibiotics to alleviate pain and prevent infection. Inadequate to treat the illness, home therapies like saline rinses help promote recovery and offer some palliative relief. Dentists must administer dental treatment promptly to guarantee optimal recovery and appropriate care.
Will dry socket heal itself?
Yes, a dry socket heals itself. A dry socket heals itself over time, but the process is slow and painful without intervention. Granulation tissue, a combination of new connective tissue and microscopic blood vessels, is produced by the body during the healing process. The tissue is formed on the surfaces of a wound. The socket is progressively filled with granulation tissue, covering the exposed bone and nerves, providing protection and promoting new bone and gum tissue growth. The absence of a protective blood clot significantly prolongs the healing process and elevates the likelihood of infection and severe pain. Dental treatment must be pursued to expedite healing, prevent complications, and manage symptoms.
How do Dry Socket Affect Wisdom Tooth?
A dry socket affects a wisdom tooth by inducing excruciating pain and complications that impede post-extraction recovery. A hemostatic clot usually forms at the wisdom teeth extraction site to protect the surrounding nerves and osseous tissues. The clot either dislodges or does not grow enough, exposing the bone and neural tissues in a dry socket. The exposure precipitates intense pain that radiates to the auricular, ocular, or cervical regions on the same side as the extraction, making it a particularly aggravating problem with wisdom tooth extractions.
Dry socket wisdom teeth present unique challenges due to the anatomical positioning and complexity of extracting third molars. Wisdom teeth, the terminal set of molars, are more arduous to extract, elevating the risk of dry socket development. The difficulty in sustaining optimal oral hygiene in the posterior region of the oral cavity and the propensity for food particles and bacteria to lodge in the extraction site further exacerbate the situation. The condition intensifies the pain and extends the convalescence period, rendering dry socket wisdom teeth an incredibly protracted and painful ordeal.
The problem with wisdom tooth dry socket is not confined solely to pain; it augments the risk of infection. The exposed osseous structures and nerves are susceptible to bacterial colonisation, heightening the risk of infection. It manifests as swelling, pyrexia, and additional discomfort, further complicating the recovery.
What are the Researches about Dry Socket?
The researches about dry socket evaluate the effectiveness of interventions like chlorhexidine rinses, platelet-rich plasma, smoking cessation, and low-level laser therapy in prevention and treatment, and understanding its causes and improving treatments.
The Cochrane Review titled "Chlorhexidine in the Prevention of Dry Socket," updated in 2021, evaluated the efficacy of chlorhexidine mouth rinses and gels in mitigating the incidence of dry sockets. The evaluation covered 49 trials totalling 6771 participants and found that 39 trials centred around prevention and ten around treatment. The findings revealed that chlorhexidine rinses (0.12% and 0.2% concentrations), administered before and 24 hours post-extraction, significantly curtailed the risk of dry socket development, with an odds ratio (OR) of 0.38 compared to placebo. Applying chlorhexidine gel intrasocket post-extraction reduced the odds of dry sockets by 58% (OR 0.44), underscoring its preventive efficacy.
The systematic review titled "Is There a Relationship Between Smoking and Dry Socket?" sought to elucidate the correlation between tobacco use and the prevalence of dry sockets. The meta-analysis incorporated eleven studies conforming to PRISMA guidelines, revealing that smokers exhibited more than threefold increased odds of developing dry sockets post-extraction compared to non-smokers. The aggregated incidence was approximately 13.2% in smokers versus 3.8% in non-smokers, signifying a substantial link between smoking and heightened dry socket risk.
The review "Treatment Approaches for Dry Socket" examined a spectrum of therapeutic modalities for dry socket management over two decades, analysing 3857 results and meticulously selecting 17 articles. Therapeutic interventions were classified into empirical, conventional, and regenerative strategies. Traditional treatments emphasised analgesia, infection prophylaxis, and inflammation mitigation, whereas contemporary approaches like Platelet-Rich Plasma and laser therapy focused on promoting angiogenesis and granulation tissue formation. The review's evidence supports the superior efficacy of regenerative treatments, although conventional methods continue to be prevalently employed.
The study "Efficacy of Low-Level Laser Therapy (LLLT) in the Management of Dry Socket" at the University Dental Hospital Sharjah investigated LLLT's role in ameliorating dry sockets. The results showed that LLLT significantly lowered pain levels and accelerated the production of granulation tissue compared to conventional therapy. The 45 patients were divided into two cohorts, one receiving traditional treatment and the other LLLT. The LLLT-treated cohort showed improved granulation tissue and much-reduced pain ratings (1-2) by the fourth day, confirming the therapeutic effectiveness of LLLT in promoting dry socket healing.
What are the Differences between Dry Socket and Mouth Ulcers?
The differences between dry socket and mouth ulcers are significant regarding their causes, symptoms, and treatment. Dry socket, or alveolar osteitis, occurs after tooth extractions when the protective blood clot is dislodged, exposing bone and nerves. Factors like smoking, traumatic extractions, and inadequate care cause it. Mouth ulcers, or canker sores, are small, painful lesions inside the mouth caused by stress, injuries, acidic foods, vitamin deficiencies, and health conditions like Crohn’s disease.
A dry socket is characterised by severe pain a few days post-extraction, visible bone, foul odour, bad breath, and swelling. Mouth ulcers present as round sores with a white or yellow centre, causing stinging or burning, especially when eating or talking, but without exposed bone. A dry socket treatment requires professional dental care, including cleaning the socket, medicated dressings, pain management, and antibiotics if infected. Mouth ulcers are managed at home with topical treatments, good nutrition, and avoiding irritants, though severe cases need medical attention. A dry socket and mouth ulcers cause significant oral discomfort and benefit from good oral hygiene and avoiding irritants. A dry socket needs professional intervention, while mouth ulcers are self-limiting and managed with home care.